

Male Pattern Baldness: A Dermatologist’s Guide to Early Detection and Treatment
August 27, 2021 2025-04-25 4:46Male Pattern Baldness: A Dermatologist’s Guide to Early Detection and Treatment
As an Amazon associate, Dermatocare earns from valid purchase made by clicking on the affiliate links in this blog.

Male Pattern Baldness: A Dermatologist’s Guide to Early Detection and Treatment
Male Pattern Baldness (MPB), or Androgenetic Alopecia, is the most common cause of hair loss in men, affecting nearly 50% by the age of 50. Though it follows a genetic and hormonal basis, the psychological and aesthetic impact on affected individuals can be significant. Fortunately, early intervention can slow progression and in many cases, offer partial restoration.
This article provides an in-depth understanding of the causes, clinical staging, progression patterns, predictive indicators of severity, and treatment options based on the stage of baldness.
Why Does Male Pattern Baldness Occur?
The primary trigger for MPB is Dihydrotestosterone (DHT), a metabolite of testosterone, which acts on genetically sensitive hair follicles.
The DHT Pathway:
- Testosterone is converted into DHT via the enzyme 5-alpha reductase (Type II) in hair follicles.
- DHT binds to androgen receptors in hair follicle cells, particularly in the frontal, temporal, and vertex scalp areas.
- In genetically predisposed individuals, this leads to:
- Shortening of the anagen phase (growth phase)
- Progressive miniaturization of the hair follicle
- Transformation of thick terminal hairs into thin vellus hairs
- Eventual cessation of hair production
The occipital scalp typically retains hair due to its relative resistance to DHT, which also makes it a viable donor area for hair transplantation procedures.
Stages of Male Pattern Baldness: Norwood-Hamilton Classification
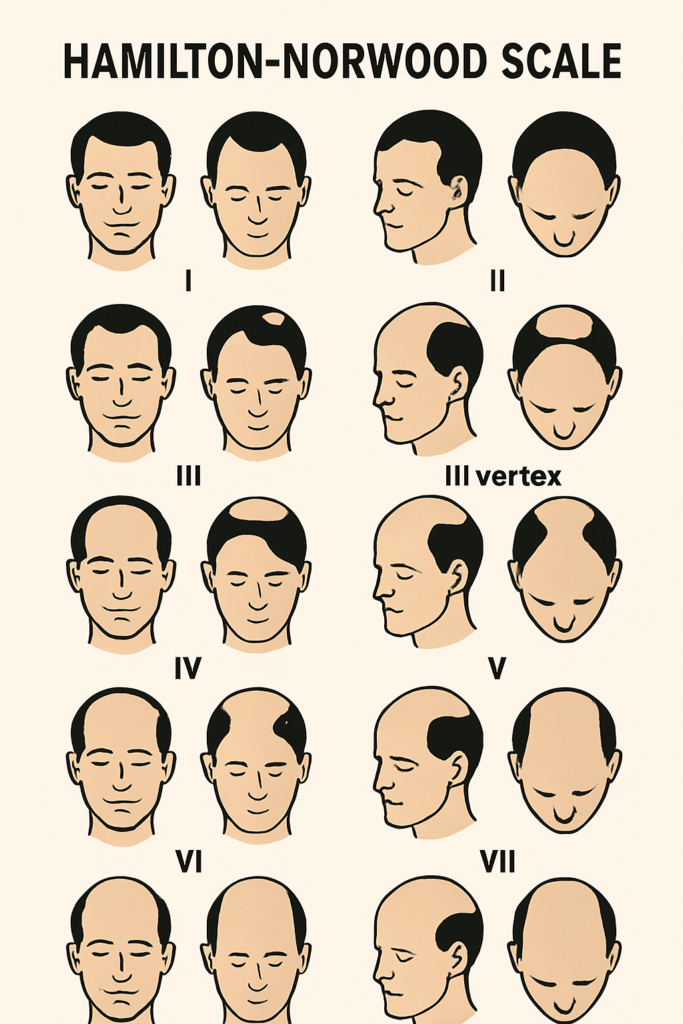
The severity and progression of male pattern baldness is classified by the Hamilton-Norwood scale, which dermatologists use for treatment planning and monitoring:
| Stage | Pattern of Hair Loss |
|---|---|
| Stage 1 | Minimal or no recession of the hairline |
| Stage 2 | Early recession at the temples, typically symmetrical |
| Stage 3 | Deep temporal recession, often the first stage of clinical baldness |
| Stage 4 | Frontal and vertex balding separated by a band of hair |
| Stage 5 | The separating band becomes narrower; frontal and vertex balding areas enlarge |
| Stage 6 | The bridge disappears, forming a single large bald area |
| Stage 7 | Only a horseshoe-shaped rim of hair remains on the sides and back |
Onset can vary from as early as 19 years to as late as 55 years. It is a slowly progressive condition that may take decades to reach the advanced stages, although rapid progression over 1–2 years can occur in some individuals.
How to Know If It Will Be Severe?
Indicators of severe or rapid progression include:
- Early onset (before 25–30 years)
- Noticeable hair thinning within a year
- Positive family history of severe baldness
- Trichoscopic evidence of miniaturized follicles
- Visible scalp despite average hair length
- Widening vertex area
Identifying these signs early enables prompt initiation of therapy, improving treatment outcomes.
When to Start Treatment?
Early intervention is crucial. Treatments are most effective when miniaturization has started but follicles remain alive. Once complete follicular atrophy has occurred (Stage 6–7), only surgical options like transplantation may offer meaningful restoration.
Treatment
Stage 1–2 (Preventive phase)
- Topical Minoxidil 5%
- Low-Level Laser Therapy (LLLT)
- Nutritional support (biotin, vitamin D, iron, zinc)
Laser therapy is effective only in the early stages when hair loss is minimal. It is ineffective in cases of advanced or complete baldness. Home-use devices include combs, brushes, or caps. Clinical-grade laser helmets or hoods are used in restoration clinics.
Stage 3–4 (Active treatment phase)
- Combination therapy: Minoxidil + Finasteride
- Microneedling with PRP or Growth Factors
- Oral Dutasteride in selected cases
- Trichoscopic monitoring and response tracking
PRP and mesotherapy are suitable in the early stages of baldness, especially in patients unresponsive to first-line treatments like Minoxidil and Finasteride.
Stage 5–6 (Advanced phase)
- Continue pharmacological agents to preserve remaining follicles
- Evaluate for Hair Transplant Surgery
- Scalp camouflage techniques like dermal fibers or micropigmentation
- Ideal candidates are those with significant baldness in the frontal, mid-scalp, or crown areas but with good donor density on the sides and back.
Stage 7 (End-stage baldness)
- Hair Transplantation becomes the primary restorative option
- Consider scalp micropigmentation, hair systems, or wigs if transplant is not feasible
Conclusion
Male pattern baldness is a chronic, progressive condition. The window for maximal therapeutic benefit lies in the early stages, when follicular viability remains. Timely diagnosis, objective staging, and a customised treatment protocol—medical or procedural—can dramatically alter the long-term aesthetic and psychological impact of baldness.
Do not wait for extensive thinning. The earlier you act, the higher your chances of preserving and restoring your hair.
Use the Dermatocare Regime Finder Tool to discover a personalised hair regrowth regime tailored to your stage of male pattern baldness. This tool recommends evidence-based, dermatologist-approved solutions to optimise your hair recovery journey.
ROUTINE FINDER
Get free dermatologist-recommended regime by choosing your skin or concerns.

FACE

HAIRS

CHILD

BODY



